Expanding the ACD Phenotype
Baylor published an article in the November 2004 Journal of Pediatrics entitled “Expanding the Phenotype of Alvelolar Capillary Dysplasia”. Dr Bejjani and Dr. Sen presented a summary of their research and findings at the Annual Meeting of the American Society of Human Genetics held in Baltimore on October 15-19, 2002. You can access the various sections of this through the links below, but please remember that this is a presentation for the medical community and as such is written in a very technical manner. If you have any questions or comments, please contact Dr. Pawel Stankiewicz.
| Table of contents |
|---|
| Abstract |
| Introduction |
| Subject Enrollment and Data Collection |
| Pathology |
| Results |
| Discussion |
| References |
Abstract
Alveolar Capillary Dysplasia (ACD) is a rare and lethal developmental anomaly of the pulmonary vasculature. It is generally described as the failure of formation of the normal air-blood diffusion barrier in the newborn lung.
ACD is usually associated with misalignment or displacement of the pulmonary veins. The disease presents very early in infancy, usually after a few hours of normal breathing. Infants become critically ill very rapidly in the first days of life with severe hypoxemia and pulmonary hypertension. There is no cure for ACD. The disease is uniformly lethal. Standard therapies include mechanical ventilation, high concentrations of inspired oxygen, inhaled nitric oxide and ECMO support. These therapies may prolong life by days to weeks, but have led to no long-term survival.
We have established a close working relationship with the ACD Association, the only parent support organization and have already collected 29 families, each with one or more infant with ACD in preparation for positional mapping and eventually cloning the ACD gene(s). Clinical records and pathological samples from affected individuals, and DNA from affected and unaffected individuals were obtained. Our review of the pre and postmortem records of 24 affected individuals allows us to define better both the natural history of this condition and the associated anomalies with the ACD phenotype. Our collection of families corroborates the possible recessive nature of this condition and provides additional data for genetic and prenatal counseling.
Analysis of the various associated anomalies allows us to formulate a hypothesis regarding possible candidate genes and/or signaling pathways. The material collected here represents the largest cohort of ACD patients ever assembled. It also allows for positional mapping of the putative ACD gene as a first step towards understanding this condition. Perception of the clinical spectrum of ACD and cloning the responsible “gene”, have implications for counseling, for prenatal testing, and for comprehending the molecular pathophysiology of ACD and other organ malformations that are associated with this condition.
Introduction
Persistent pulmonary hypertension of the newborn (PPHN) is the most common cause of death in normally formed infants in the United States with an incidence of 1 in 1,400 live births [1]. PPHN may be a manifestation of one of many primary conditions including fetal hypoxia, pulmonary hypoplasia, congenital heart disease, pneumonia, sepsis, or respiratory distress associated with prematurity.
H. Edward MacMahon (1947) described an uncommon neonatal lethal cause of PPHN, which he termed “Congenital Alveolar Dysplasia of the Lungs” [2]. He also documented its association with developmental anomalies in other organs [2]. These findings were similar to those described by Janney et al. [3]. In addition, they described a remarkable paucity of alveolar capillary membranes and an abnormal venous pattern [3] and named this condition “Congenital Alveolar Capillary Dysplasia”. Additional case reports supported the significance of misalignment of the pulmonary vessels [4,5]. The probable autosomal recessive nature of the condition was suspected based on reports of multiple affected siblings born to consanguineous parents [6,7].
Subject Enrollment
Affected study subjects and their first-degree relatives were ascertained through the ACD Association, a parent support organization and through contacts with pathologists and genetic counselors. The Baylor College of Medicine Institutional Review Board (IRB) approved the consent forms in accordance to NIH guidelines. Biological specimens (lung tissue, paraffin embedded tissue from lung and other organs) were obtained from study subjects and blood was obtained from their unaffected relatives after the appropriate consent forms were signed.
Data Collection
Referred patients were enrolled in the study after review and independent confirmation of the pathological diagnosis by one of the authors (C.L.).
Medical and hospital records including autopsy reports were analyzed. DNA was obtained form paraffin blocks obtained from affected and deceased individuals, and from all first-degree relatives available.
Pathology
- Malposition of pulmonary vein branches (misalignment)
- Severe medial hyperplasia, small pulmonary arteries
- Defecient alveolar development
- Deficient capillary development
- Lymphangiectasis (~ 1/3rd cases)
Results
Our review of the pre and postmortem records of affected individuals allows us to define better, not only the natural history of this condition, but also the associated anomalies with the ACD phenotype. Further, analysis of the various associated anomalies allows us to formulate a hypothesis regarding possible candidate genes and/or signaling pathways.
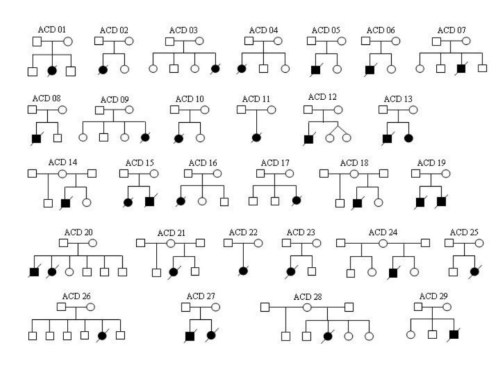
We have collected 29 families, each with one or more infants with ACD in preparation for positional mapping and eventually cloning the ACD gene(s) (see diagram below).
Clinical records and pathological samples from affected individuals were obtained and analyzed from 24. The table below summarizes the clinical and pathological findings in these individuals. Seventy four percent of the affected individuals have major organ malformations. These include defects in the urogenital system, malrotation of the intestine, defects in the heart development among others. Most pregnancies were term and uncomplicated. However, a small percentage of the cases had oligohydramnios. Average life span was 24.7 days.
| Patient # | GA | BW | AD (days) | Sex | CV | Lungs | GI/Spleen | GU | Other |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Term | ? | 22 | F | PFO | ACD | Maformation | NL | None |
| 2 | 40 | ? | 27 | F | PFO | ????ACD | NL | NL | |
| 3 | 1 | M | NL | ACD | Hepatosplenomegaly | Obstruction | |||
| 4 | 38 | 4270 | 7 | F | NL | ACD | Malformation | Obstruction | |
| 5 | 38 | 3017 | 22 | M | NL | ACD Plus | Limited Autopsy to Heart and Lungs Only | ||
| 6 | 39 | LGA | 10 | M | CHD | ACD | Microvesicular Steatosis | Obstruction | |
| 7 | 38 | 3295 | 4 | M | NL | ACD | NL | Obstruction | Prenatal DX of Oligo.Limited Autopsy to Lungs, Kidneys, Bladder and Urethra Only |
| 8 | 40 | 17 | M | PDA | ACD | Malformation | NL | ||
| 9 | Term | 3600 | 2 | F | PFO, PDA | ACD | Malformation | ||
| 10 | 39 | 22 | M | NL | ACD | Congestive Hepatomegaly | Obstruction | Prenatal Dx Of Oligo, Hydronephrosis and Pulm Hypoplasia | |
| 11 | Term | 3850 | 5 | F | CHD | ACD | Not Examined | Clinically Normal. No Path Exam Performed | Limited Autopsy to Heart and Lungs only |
| 12 | Term | 9 | F | PDA, PFO | ACD Plus | Malformation | Clinically Normal. No Path Exam Available | No Brain Path Performed | |
| 13 | 32 | 10 | M | CHD | ACD Plus | Malformation | Obstruction | Prenatal Dx of Polyhydramnios | |
| 14 | 36 | 3120 | 33 | F | NL | ACD | NL | NL | None |
| 15 | Term | 12 | M | NL | ACD | NL | NL | None | |
| 16 | 41 | 2790 | 19 | F | N/A | ACD | N/A | N/A | N/A |
| 17 | Term | 2900 | 21 | M | PDA, PFO | ACD | Malformation | NL | None |
| 18 | Term | 3595 | 30 | F | Absence Of Left Umbilical Artery | ACD | Malformation | NL | 46,XX |
| 19 | N/A | N/A | N/A | F | N/A | N/A | N/A | N/A | No Autopsy Performed. |
| 20 | Term | 87 | M | NL | ACD PLUS | Moderate Hepa Tosplenomegaly | NL | ||
| 21 | Term | 3460 | 113 | F | CHD | ACD | NL | NL | Limited Autopsy to Heart and Lungs Only |
| 22 | 38 | 3267 | 14 | F | Not Examined | ACD | Not Examined | Not Examined | Sturge-weber Syndrome. Limited Post Mortem to Lung Biopsy |
| 23 | 16 | F | NL | ACD | Not Examined | Not Examined | Limited Autopsy to Heart and Lungs only | ||
| 24 | 2435 | M | NL | ACD | NL | Obstruction | Has a Similarly Affected Sib. |
Discussion
The co-occurrence of lung, gut, heart, and GU anomalies in these patients suggest that the genetic defect that causes ACD also affects normal development of these other organs. Also, the presence of ACD in siblings born to consanguineous parents suggests a recessive mode of inheritance, although a dominant defect with decreased penetrance, or with parental gonadal mosaicism cannot be excluded.
Important genes involved in the normal development of the pulmonary, gastrointestinal, renal and cardiovascular systems would be possible candidates. These would include genes that code for a variety of secreted factors such as Fibroblast Growth Factors (FGF) and Bone Morphogenetic Proteins (BMPs; with BMP4 being the most interesting candidate) or for transcription factors such as a number of HOX genes or many genes that are targets of Sonic Hedgehog (SHH) signaling pathway.
Our review of the pre and postmortem records would define better both the natural history of ACD and its associated anomalies, providing additional data for genetic and prenatal counseling. Finally, the material collected would allow positional mapping of the putative ACD gene as a first step towards understanding the molecular mechanism underlying this condition.
References
- Inhaled nitric oxide for the early treatment of persistent pulmonary hypertension of the term newborn: a randomized, double-masked, placebo-controlled, dose-response, multicenter study. The I-NO/PPHN Study Group. Davidson D, Barefield ES, Kattwinkel J, Dudell G, Damask M, Straube R, Rhines J, Chang CT. Pediatrics 1998;101:325-34
- McMahon HE, Congenital alveolar dyslplasia: developmental anomaly involving pulmonary alveoli. Pediatrics, 1948; 2: 43-57.
- Janney CG, et al. Congenital alveolar capillary dysplasia-an unusual cause of respiratory distress in the newborn. Am J Clin Pathol. 1981;76:722-727.
- Vassal HB, et al. Familial persistent pulmonary hypertension of the newborn resulting from misalignment of the pulmonary vessels (congenital alveolar capillary dysplasia). J Med Genet. 1998 Jan;35:58-60.
- Wagenvoort CA. Misalignment of lung vessels: a syndrome causing persistent neonatal pulmonary hypertension. Hum Pathol. 1986;17:727-30.
- Boggs S, et al. Misalignment of pulmonary veins with alveolar capillary dysplasia: affected siblings and variable phenotypic expression. J Pediatr. 1994;124:125-8.
- Gutierrez C, et al. Congenital misalignment of pulmonary veins with alveolar capillary dysplasia causing persistent neonatal pulmonary hypertension: report of two affected siblings. Pediatr Dev Pathol. 2000;3:271-6.
- Langston C. Misalignment of pulmonary veins and alveolar capillary dysplasia. Pediatr Dev Pathol. 2000;3:271-6.
